By Brian Diaz
Since I started practicing as a physical therapy clinician in 2000, the prevalence of hip pain pathologies has progressively gotten worse across all ages. This nationwide trend started to gather the attention of orthopedic physicians and has sent several to specialize in the field of hip morphology and arthroscopy. Imaging techniques have improved dramatically and allow us to recognize deformities in the hip. What has become known as pistol grip deformity, or cam impingement, and pincer impingement are regular findings on x-ray and MRI reports. Some more advanced imaging, such as a high resolution MRI or MRI with a radioactive dye, can also find a labral tear or disruption inside the hip. Various opinions on the topic from surgeons all over the world have left controversy on how to approach these findings and what it means for the long term aging process and if these lead to an increase in arthritic changes or the likelihood of a total hip replacement later in life.
Part of the reason why hip pain is being seen more and more in younger active populations is the intensity and frequency of the activity being performed. Younger generations are often driven to specialize in running and cycling at earlier ages to be competitive in their disciplines. Furthermore, the amount of training that they expose their bodies to and push through compounds the hip issue even more so they repetitively aggravate the painful area. All of this makes sense, as a practitioner, when given a visual picture of the pathology and why the repetitive nature of being an endurance athlete increases the damage.
The harder issue for me to wrap my head around is why some patients have significant complaints of pain, while others have none. A large comprehensive study out of Copenhagen in 2008 looked at 4,000+ asymptomatic hips and found the prevalence of cam deformity in approximately 17% of men and 4% of women studied. Those percentages were similar to those reported in a 2010 study published in The Journal of Bone and Joint Surgery, which looked at 200 total asymptomatic subjects, and reported that 25% of the men had the prevalence of the cam impingement and 5% of the women.
The results of the prevalence of cam impingement in asymptomatic subjects were startling and got me thinking, maybe it’s only the patients that demonstrate labral involvement that are in pain? Acetabular tears of the labrum must be the defining characteristic of hips that are in pain versus ones that exercise pain-free, right? A recent study that was published in 2015 looked at 70 asymptomatic volunteers and found on the MR scans that nearly 40% had a diagnostically confirmed labral tear.
What does this mean? How does this information help us make an informed decision of whether or not to surgically repair the hip? And will this ultimately lead to degenerative changes later in life? A study in the The Journal of Bone and Joint Surgery published in 2011 followed 96 patients ages 16 to 65 that were diagnosed with either cam, pincer, or combined (both cam and pincer) impingements and nearly 82% of the hips remained arthritis free for an average of 18.5 years. The remaining 18% developed arthritis at an average of 12 years. For the ones that did develop arthritis, was this their normal progression regardless if they had impingement or not?
The articles and studies are endless, and mounting. You can spend hours pouring over the literature to find the one article that supports your case or is against it and still won’t feel complete. So let’s take a more comprehensive look and determine what options are out there if you are still unsure that surgery is the fix.
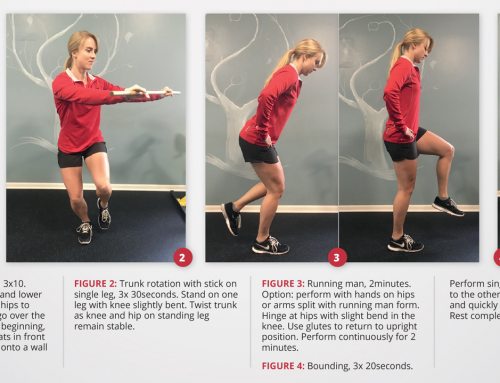
The hip joint is very similar to another ball and socket joint, the shoulder, so why not treat it similarly? With the shoulder, if we have a problem with the labrum – mostly occurring in overhead athletes that have also developed a tear due to overuse – we first try and activate some of the surrounding joint muscles to decrease the stress on the joint and improve it’s dynamic stability. The hip is no different. For those that do have femoral acetabular impingement (FAI) and are symptomatic and in pain, regardless of whether or not there is labral involvement, we try to correct the muscle imbalance. Tightness in the quadriceps, adductors, and tensor fasciae latae (TFL) needs to be addressed. Weakness in the posterior chain, in particular the glutes needs to be corrected. We pour our energy into strengthening, stretching, and mobilizing these areas and over time, months and perhaps even over a year, the changes will start to result in a more permanent decrease in symptoms.
If all of that does not work and steroid shots give no relief, then, there is surgery. Despite the above referenced articles, some people have advanced to the point where exercises and soft tissue work are no longer helping and surgery becomes inevitable. Surgically, they go in through a series of portals arthroscopically to get to the hip. Distraction of the hip joint allows even greater access to the labrum and the surgeon can repair the tear or remove the disruption to the labrum while grinding down the impingement to make a more rounded and congruent joint. This process is very involved and could take a couple of hours or more in the OR. After months of physical therapy and rehabilitation, hopefully, the hip is restored back to normal.
In summary, the prevalence of hip pathology is on the rise and most likely will only get worse. The taxation and amount of exercise we are putting on the body as endurance athletes is bound to create problems. Combined with a deformity of the hip and possible labral involvement, this could be the perfect storm to cause an increase in pain if you continue to ignore the signs and symptoms. Some of you are also time-crunched and the thought of adding hours of exercises and soft tissue work to an already busy day is exhausting. Sometimes 1-2 hours a day of exercises and stretches for the rest of the foreseeable future is life altering enough to consider surgery. At the end of the day, the decision is yours and yours alone. After 3 years of exercises and conservative management, I too, was faced with the decision of surgery and will address my experience in a forthcoming article next month. Unfortunately, will the rise of popularity of triathlons, cycling, and ultra marathons, the prevalence of people making these decisions is likely to increase.
# # #
Brian Diaz is the head physical therapist and sports specialist at ActivEdge Fitness & Sports Performance. He is a Level II Certified TRX Suspension Trainer and a USA Triathlon Certified Coach. Follow him on Twitter (@JediTriathlete) or go to his website at ExperienceTheEdge.com for more exercise ideas.